1801006052 Long case
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 13 year old female patient resident of Suryapet presented to OPD with
CHIEF COMPLAINTS
Vomitings since 1 day
Shortness of breath since 1 day
HISTORY OF PRESENTATION ILLNESS
Patient was apparently asymptotic till the age of 11years
She was sent to hostel for studies
After few days of hostel stay she noticed that bilateral swellings over the neck 5-6 in number
History of fever which is insidious in onset,intermittent, not associated with chills and rigors no evening rise of temperature
History of cough which is intermittent and not associated with any sputum
for which she was taken to RMP, he has initiated her on ATT as her mother has also has Tuberculosis
They used ATT for 2months started in the month of June 2021
After initiating ATT fever was increased so they discontinued ATT and was referred to Hyd by the RMP
Patient was taken to hospital where she was evaluated for tuberculosis but was tested as negative for Acid fast bacilli, culture,cbnaat. ,she also complained of bilateral knee and wrist joint pains.
In hospital they suspected it to be autoimmune and started her on Tab Wysolone and Tab HCQ ,which she used for 15 days and stopped.
Patient was tested for -
ANA ELISA-equivocal,ANA IFA-negative
Anti Ds DNA ELISA-Positive,Anti Ds DNA IFA negative.
She was taken to another local hospital with c/o joint pains,facial puffiness,pedal edema,fever ,cough
Lymph node biopsy was done in the month of May 2022
Mycobacterial gene expert test was done and was confirmed with Tuberculosis and was started on ATT for 6 Months.
Before starting ATT attendors had noticed that she is developing facial rash ( black in colour) rash all over the body and Hair loss.

Patient was fine till the month of January 2023 ,she developed generalised edema due to proteinuria.
Fever was on and off from then which got relieved on taking medication.
Pedal edema since 2 weeks till the level of knee, Abdominal distension since 1 week .
March 13: She had Vomitings 4 -5 episodes non bilious ,food as content.
Shortness of breath of grade 2
PAST HISTORY:
Patient is a known case of Tuberculosis, diabetes, Hypertension, epilepsy,asthma.
PERSONAL HISTORY:
Daily routine - Patient wakes up at 7 am does her daily routine work , previousy she used to stay at hostel ,goes to school at 9 am ,lunch at 1 pm ,comes back from school take some snack ,playtime till 6 pm, dinner at 7 :30 pm and goes to sleep at 10 pm .
Now patient wakes up at 7 am does her routine work,take break fast at 9 am and takes rest lunch at 1 pm ,snacks ,fruits at 4:30 ,8 pm dinner,9 pm sleep.
Appetite - decreased.
Diet - Mixed
Bowel and bladder movements: patient complained of decreased urine output,bowel movements are normal .
Sleep: inadequate
FAMILY HISTORY:
Mother is a known case of Tuberculosis ,died 6 months ago
BIRTH HISTORY: She is the first child born out of 2nd degree consanguineous marriage

MENSTRUAL HISTORY
Not attained menarche .
GENERAL EXAMINATION:
Patient is conscious coherent and cooperative ,well oriented to time place and person poorly built and moderately nourished .
Pallor present
Icterus absent
Cyanosis absent
Clubbing absent
Lymphadenopathy absent
Bilateral pedal edema present

Vitals:
Temperature
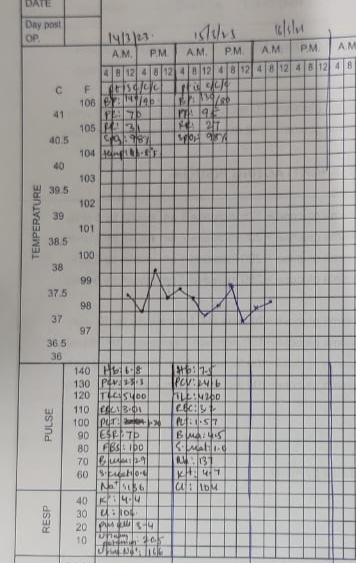
Pulse rate:88beats /min
Blood pressure:130/70
Respiratory rate:22cycles per minute.
SYSYTEMIC EXAMINATION:
Abdominal examination:
Inspection:
Shape - slightly distention.
Umbilicus - Inverted
No visible pulsation,peristalsis, dilated veins and localized swellings.
Palpation:
soft, tenderness in right and left Hypochondrium, epigastrium.
Percussion:
shifting dullness present.
Auscultation:
Bowel sounds heard
Respiratory examination:
Bilateral air entry present
Dull note heard on percussion
Vocal resonance decreased.
Cvs examination
S1 s2 heard, no murmurs
Jugular venous pressure:
https://youtube.com/shorts/nx6XLEUBxJY?feature =share
CNS examination:
No focal neurological deficits
Higher mental functions normal
Cranial nerves normal
Sensory examination normal
Motor examination normal
Reflexes normal.
INVESTIGATIONS:
14/03
Serum electrolytes:
Sodium 136 meq/l
Potassium 4.4 mEq/l
Chloride 106 meq/l
Serum creatinine 0.6mg/dl
Esr 70 mm
CRP neagtive
Blood urea 29 mg\dl
FBS 100 mg\dl
Blood group 0+
Rheumatoid factor negative
HIV non reactive
Hbs ag non reactive.
COMPLETE URINE EXAMINATION:
Colour pale yellow
Appearance: clear
Acidic
Specific gravity 1.010
Albumin ++
RBC: 4-6
No sugar, bile salts, bile pigments, casts, amorphous deposits
Pus cells 3 to4 \hpf
Epithelial cells 2 to 3 \hpf
ULTRASOUND ABDOMEN:
Liver,gallbladder,pancreas,spleen, uterus,ovaries normal
Moderate ascites
Bilateral pleural effusion
Moderate pericardial effusion
Bilateral grade 2 rpd change
COMPLETE BLOOD PICTURE:
14/03:
Hb- 6.8g%
Wbc-5,400
Platelet:1,20,000
Pcv:23.3
MCv:77.4
Mch:22.6
Mchc:29.2
Rdw:20.1
RBC:3,01
Smear- Anisopoikilocytosis,with microcytes ,tear drop cells ,pencil forms.
15/03:
COMPLETE BLOOD PICTURE:
Hb 7.5 g\dl
WBC 4200 cells\cumm
Neutrophils 60
Lymphocytes 36
Eosinophils 02
Monocytes 02
Basophils 0
Pcv 24.6 vol%
Mch 76.4 fl
Mchc 30.5%
Rdw 20.6 %
Rbc count 3.2 million\cumm
Platelet 1.57 laksh\cumm
Smear normocytic normochromic anemia
16/03:
Hb-7.2g%
Pcv-23.7
Mcv-70
Mch: 22.1
Mchc:20.4
Rdw:20.
15/3:
Serum creatinine 1.0 mg\dl
Serum electrolytes:
Sodium 1.37 meq\l
Potassium 4.7
Chloride 104
Spot urine protein :393 mg\dl
Spot urine creat 37.8 mg\dl.
Chest X ray:

ECG:








TREATMENT:
Fluid restriction
Salt restriction
Inj lasix 40mg IV BD
Inj monocef 1gm IV BD
Inj Methyl prednisolone 250mg in 100ml NS IV OD
Tab Aldactone 25mg PO OD
Tab shelcal 500mg PO OD
Vitals monitoring .
posted by 54 Harika Kathumandi @ March 16, 2023
![]()

<< Home