Altered sensorium secondary to hypoglycemia , dyselectrolytemia.
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
A 65 year old female patient resident of Nalgonda Telugu tutor by occupation was bought to casualty with chief complaints of altered behaviour for an hour in the morning on28/11/2022
History of presenting Illness:
Patient was apparently asymptomatic 20 years back then she developed Bilateral Hip and knee pains which was insidious in onset gradually progressed aggravated on doing work and relieves temporarily on taking medication ,she stopped working as Telugu tutor because of the pain.
Patient developed diminision of vision in Right eye since 14 years which has led to complete loss of vision 10 years back . Perception of light is present.
She took some ayurvedic treatment (unknown)for 3 years(2016-2019) after that she developed generalized edema all over the body , stopped the medication on doctor's advice.
She used pain killers once in a while
It is now progressed to such an extent that it has caused fixed flexion deformity bilaterally . Patient walks with the help of Walker since 3-5 months.
Patient was apparently asymptomatic 6 days back fever decreased on taking medication (crocin) , She had odynophagia the next day for both solids and liquids ,she hardly takes any food,she took 1-2 idli and glass of milk .
She also complained of nausea,nonprojectile vomiting with food particles as the content,non blood stained.
On 28/11/2022
Patient started shouting in the morning around 8 am ,started pulling her hair and talking irrelevantly with her family members ,after feeding two idlis she was calm for a while she was taken to the hospital around 10:30 am , patient was semiconscious and coherent on her way to the hospital.
Past History:
No similar complaints in the past .
Not a known case of Diabetes , hypertension, Tuberculosis, Epilepsy,asthma,Coronary artery disease .
Family History:
No significant family History
Personal History:
Appetite: decreased ( she always had less appetite),diet- mixed, bowel and bladder movements - regular ,sleepi is adequate and no addictions
On General examination:
Patient was semi conscious coherent and cooperative
Moderately built and nourished
pallor present

,No, Icterus, Cyanosis,
Clubbing, generalized lymphadenopathy
bilateral pedal edema


Vitals: On the day of admission -
Pulse rate: 96bpm
Blood pressure:110/70mmHg
Temperature:afebrile
Respiratory rate:20cpm
Blood Glucose:50mg/dl
At 6pm: 138mg/dl
At8pm: 181mg/dl
Systemic Examination:
Central nervous system examination :
Consciousness: conscious
GCS: E4V5M6
Orientation: oriented to place time and person
Memory:
Immediate: intact
Recent: intact
Remote:intact
Attention: intact
Calculation: intact
Cranial nerves: intact
Motor system :
Muscle tone: Right Left
UL N. N
LL N. N
Muscle power:
UL -5/5 Right 5/5 Left
LL - cannot be assessed because of Flexion deformity of lower limbs.
Reflexes
Right Left
Biceps 2+ 2+
Triceps 2+ 2+
Supinator 2+. 2+
Knee - -
Ankle - -
Superficial reflexes and deep reflexes are present , normal.
Sensory system - all sensations ( pain, touch, temperature, position, vibration sense) are normal
Mini mental status examination:19/30

Per abdomen:
Inspection:
No Abdominal distension
No scars, sinuses, mass visible

Palpation:
Inspectory findings are confirmed
No local rise of temperature
Tenderness absent
Cardiovascular system examination :
Inspection : Bilaterally symmetrical chest present
No scars, sinuses
Palpation:
Inspectory findings are confirmed
Apex beat normal
On Auscultation :
S1 S2 heard
No murmurs or additional heart sounds
Diagnosis:
Altered sensorium secondary to hypoglycaemia (recovered) with dyselectrolytemia.
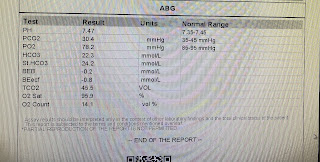
INVESTIGATIONS:



On 30/11/22

Usg Abdomen















Treatment:
1.I.v fluids 0.9%Nacl@30ml/hr
2.GRBS 6th hrly monitoring
3.BP 2 bd hrly monitoring
posted by 54 Harika Kathumandi @ December 01, 2022
![]()

<< Home